Infections and infestations: Very Common: Viral infection.
Common: Pneumonia, respiratory infection, urinary tract infection, otitis media.
Blood and the lymphatic system disorders: Common: Leucopenia.
Rare: Thrombocytopenia.
Immune system disorders: Rare: Allergic reactions (e.g. urticaria).
Metabolism and nutrition disorders: Common: Anorexia, increased appetite.
Psychiatric disorders: Common: Hostility, confusion and emotional lability, depression, anxiety, nervousness, abnormal thinking.
Rare: Hallucinations.
Nervous system disorders: Very common: Somnolence, dizziness, ataxia.
Common: Convulsions, hyperkinesias, dysarthria, amnesia, tremor, insomnia, headache, sensations such as paresthesia, hypaesthesis. Coordination abnormal, nystagmus, increased, decreased or absent reflexes.
Rare: Movement disorders (e.g. choreoathetosis, dyskinesia, dystonia.
Eye disorders: Common: Visual disturbances as amblyopia, diplopia.
Ear and labyrinth disorders: Common: Vertigo.
Rare: Tinnitus.
Cardiac disorders: Rare: Palpitations.
Vascular disorder: Common: Dyspnoea, Bronchitis, pharyngitis, cough, rhinitis.
Gastrointestinal disorders: Common: Vomiting, nausea, dental abnormalities, gingivitis, diarrhea, abnormal pain, dyspepsia, constipation, dry mouth or throat, flatulence.
Rare: Pancreatitis.
Hepatobiliary disorders: Rare: Hepatitis, jaundice.
Skin and subcutaneous tissue disorders: Common: Facial oedema, purpura most as bruises resulting from physical trauma, rash, pruritis, acne.
Rare: Stevens-Johnson syndrome, angioedema, erythema multiforme, alopecia.
Musculoskeletal, connective tissue and bone disorders: Common: Arthralgia, myalgia, back pain, twitching, throat, flatulence.
Renal and urinary disorders: Common: Incontinence.
Rare: Acute renal failure.
Reproductive system and breast disorder: Common: Impotence.
General disorders and administration site conditions: Very Common: Fatigue, fever.
Common: Peripheral or generalized oedema, abnormal gait, asthenia pain, malaise, flu syndrome.
Rare: Withdrawal reactions (mostly anxiety, insomnia nausea, pains, sweating), chest pain. Sudden unexplained deaths have been reported where a causal relationship to treatment with gabapentin has not been established.
Investigations: Common: WBC (white blood cell count) decreased, weight gain.
Rare: Blood glucose fluctuations in patients with diabetes, elevated liver function tests.
Injury and poisoning: Common: Accidental injury fracture, abrasion.
Under treatment with gabapentin cases of acute pancreatics were reported. Causality with gabapentin is unclear.
Respiratory tract infections, otitis media, convulsions and bronchitis were reported only in clinical studies in children. Additional in clinical studies in children, aggressive behavior and hyperkinesias were reported commonly.


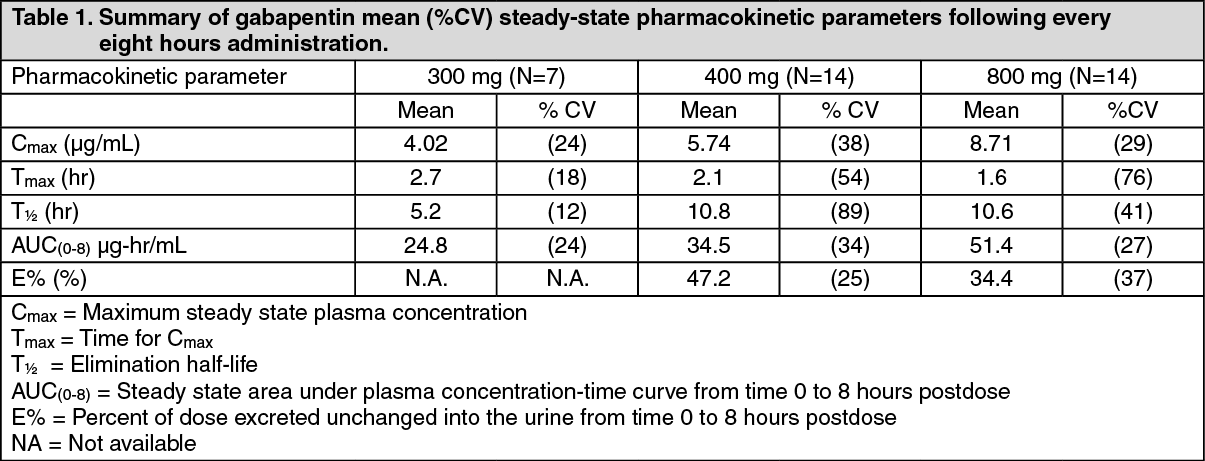 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image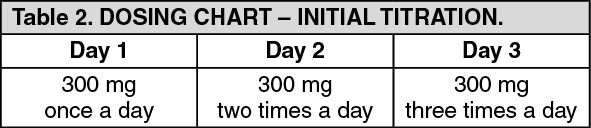 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image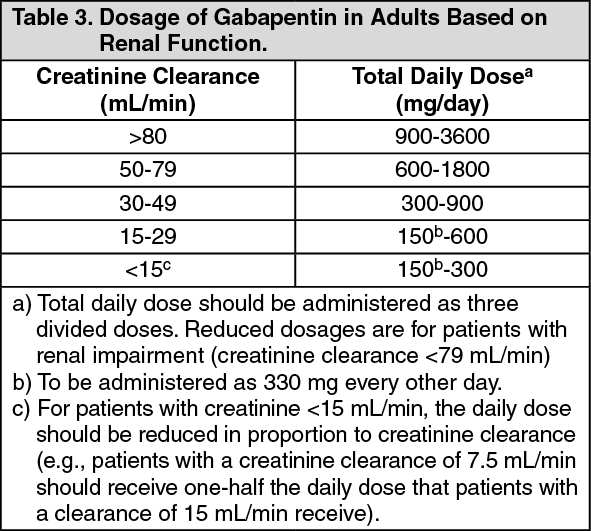 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out